
Musculoskeletal problems in target rifle shooters
 Mr Jonathan Hull MD FRCS(Orth), Consultant Orthopaedic Surgeon, Frimley Park Hospital NHS Foundation Trust, Camberley & Spire Clare Park Hospital, Crondall. ([email protected])
Mr Jonathan Hull MD FRCS(Orth), Consultant Orthopaedic Surgeon, Frimley Park Hospital NHS Foundation Trust, Camberley & Spire Clare Park Hospital, Crondall. ([email protected])
(Jonathan shoots regularly for Hampshire and was selected for England in the 2010 National match and the European Long Range Championships. He was also a member of the 2011 NRA Channel Islands Team)
Introduction
To my knowledge there are only two orthopaedic surgeons currently shooting target rifle at Bisley. Do the others know something we don’t? There are various musculoskeletal ailments that can either be brought on by shooting, or can hamper one’s performance of the sport, but fortunately these seem to be quite rare – at least they have been until this article has been read by the shooting fraternity! In order to try and help with definition of the words we use, I have put orthopaedic terms in italics and have given an explanation in the text.
I should like to present a fairly light-hearted view of orthopaedic shooting problems and offer some advice on how best to overcome any difficulties they may produce. I am also always happy to offer advice both at Bisley and by e-mail or other means; hopefully you will never need it.
Areas of concern
From an orthopaedic perspective, we think of the human frame as being a central trunk, shoulder and pelvic girdles, and the upper and lower extremities. Although problems may overlap, it is generally easier to describe ailments within these areas. Hopefully, not too many shooters will have multiples aches and pains simultaneously.
Central trunk
The trunk comprises the head, neck, and spine; midline structures, but with paired joints at every level in the spine (48 separate joints, all of which can hurt). Spondylitis is a commonly used term and refers simply to the process of wear and tear arthritis in the joints of the spine; the symptoms of stiffness and pain are common, especially in the lower back when the term lumbago is sometimes used. Sciatica is leg pain caused by pressure of a slipped intervertebral disc in the lower spine; this is usually quite severe and if present, is a good reason not to shoot until it has resolved.

Shoulder
The shoulder joint is a ball and socket surrounded by muscles known as the rotator cuff. These muscles have to pass under the end of the collar-bone and are sometimes squeezed in too tightly causing impingement. This produces pain in the shoulder and can restrict movement considerably, at its extreme leading to a frozen shoulder. Shoulder problems in shooters are quite common and can present with pain, restricted movement and a painful clicking within the joint.
Pelvis
Hip problems are common in general and as we all get older, we are prone to hip stiffness, pain and arthritis. Lying prone can be a problem with hip arthritis and may prevent good positioning. This can stop the shooter adopting the cocked leg position with his right leg, and if affecting the left leg, can stop his pelvis lying flat on the ground.
Elbow
Elbows can be a real cause of trouble for shooters. Pain and swelling over the point of the elbow is known as olecranon bursitis. This is inflammation of the soft tissue cushion which is aggravated by the pressure of lying in the prone position. Other elbow conditions such as golfers elbow and tennis elbow are also not unusual in our sport – these two expressions describe pain from inflammation of the inner and outer sides of the joint.
Olecranon Bursitis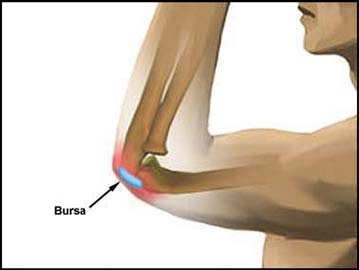 Painful swelling
Painful swelling
Knees and feet
Fortunately we lie down to shoot, and lower limb orthopaedic problems with the exception of hips are usually solved by lying flat. Getting to the correct firing point on time may, however, be an issue for the lame!
Advice and suggestions - Exercises
I cannot provide a comprehensive guide to deal with all potential problems, but I will attempt to offer some particular advice for some of the common orthopaedic ailments affecting those who shoot.
Warm ups
It is very sensible to spend a few minutes warming up each time you shoot. Just as cats and dogs stretch when they first get up after a sleep, we ought to do so after resting, especially as we get older. Joints need to move and putting the major joints through a full range of movement is always useful.
The following was written by Jackie Davies who was team physiotherapist for the GB Palma Team before emigrating to Canada (reproduced with permission):
“The method of stretching hasn’t changed much in the last 30 years, with the general consensus being that a stretch should be held for a minimum of 20 seconds (30 seconds preferable) and repeated at least 3 times. To maintain flexibility, the stretching should be done once daily. To improve flexibility, stretching should be done at least twice if not three times daily.
Stretching should be targeted at the correct structure (most commonly a muscle or a group of muscles) and should not be painful. If done well, the sensation should start as a light pull, which should ease off during the 30 seconds and allow further application of the pull (leaning more into the stretch). After stretching, the body part should feel more supple. However, this may last only a short time initially. To achieve permanent lengthening, research suggests that it can take 6 weeks of targeted stretching.”
(As in most things orthopaedic, physiotherapists usually know more than surgeons, and Jackie certainly understands the issues facing rifle shooters.)
 Spine
Spine
Anyone who has suffered with back pain and has seen a physiotherapist for it will know what exercises to do and what good effect they can have. For the amateur back pain sufferer however, the following is a simple regime worth considering when time and space allow:
Simple extensions
Stand with feet shoulder width apart and gently arch the lower back aiming to look directly upwards. Stretch backwards as far as possible and hold the position for 5 seconds. Relax and repeat 5 times.
 Lumbar rotations
Lumbar rotations
Lie on your back. With alternate knees, flex at the hip bringing your knee up towards your chest. Rotate to the side, trying to bring the side of your knee as close to the ground as you can, while keeping your shoulders flat on the ground. Hold the position for 5 seconds before returning your knees to the midline, and then rotating to the other side. Repeat 5 times.
Hip extensions
Get into the all-fours position with weight evenly distributed on hands and knees. Slowly raise one leg behind you, trying to elevate the thigh to as near horizontal as possible, keeping the trunk flat, using your stomach muscles. Hold for 5 seconds and repeat with the other leg. Do 5 sets of each.
 Press ups
Press ups
Not proper ones, but from the position flat on your front, lift up on your arms arching the spine from the waist, trying to hold the position with elbows fully straight. Hold for 5 seconds and relax, repeating 5 -10 times.
All of these exercises should be undertaken slowly and in a controlled manner, with no sudden violent or jerky movements. Done carefully, they should not put you at risk of injury, however bad your back pain feels. Most people will obtain some relief of discomfort after doing them.
Shoulders
Stretches and rotations are important and worth doing regularly. Also, keeping a good erect posture, with the shoulders well-braced, will keep the rotator cuff muscles in better condition, reducing impingement. Exercises to pull the shoulders back trying to bring the elbows together behind you can help with posture.
If you experience painful clicking in the front of the joint, don’t keep making it click if you can avoid it. It is caused by an inflamed tendon snapping over the front of the shoulder and repetition can make the inflammation worse.
Advice and suggestions – Equipment
Getting in and out of your jacket can be a problem with a bad shoulder: Always try and put the bad side in first, as this causes less shoulder movement and should be less painful. Don’t be afraid to ask for assistance getting the jacket off!
There is no avoiding the shoulder with our type of shooting. If symptoms are really severe, a rest from the sport may become necessary; cortisone injections and ultimately surgery may have to be considered.
Padding is the key with elbows. Modern shooting jackets cannot incorporate thick padding, and so we have to somehow protect the elbow inside the sleeve. There are ready made devices for elbow joint protection and these may be useful. They may be quite bulky, however, and not fit inside the jacket comfortably. If the overall pressure on the point of the elbow increases, the pain will as well, and the object of the exercise is defeated.
 I have long suffered with bursitis and have developed a near perfect solution. 7 mm thick orthopaedic felt can be bought in sheets from main chemist stores. It is designed for the foot and has a sticky side which is applied to the skin.
I have long suffered with bursitis and have developed a near perfect solution. 7 mm thick orthopaedic felt can be bought in sheets from main chemist stores. It is designed for the foot and has a sticky side which is applied to the skin.
If a square of this material is cut (approx 12x12 cm), and a small hole is cut out of the centre about 2 x 2 cm, this can be stuck onto the point of the elbow with the painful swollen tip of the olecranon projecting through thehole. The support around the elbow tip relieves just enough pressure to make shooting perfectly comfortable and the relatively thin padding layer does not cause problems inside the jacket sleeve. The adhesive is strong enough to keep the felt in place for up to several days if necessary but it can be changed daily if desired.
An alternative is to use the felt pad with the sticky side stuck to a tubigrip support. This can then be turned ‘inside out’ and the padded tubigrip worn on the elbow. Although reusable and easy to use, this is less stable and can potentially move about during a shoot.
Medication
There is not a pharmacological cure for every problem but there is no doubt that simple painkillers can help. Paracetemol is a reliable safe and effective analgesic and can be taken regularly without risk. Taken as per instructions it will reduce the level of background chronic pain and will not causeharm or addiction. Paracetemol will not mask serious or significant pain.
Anti-inflammatory drugs can be very helpful for the conditions that effect shooters. Ibuprofen (Brufen) is available over the counter. Taken as instructed, full effect is unlikely unless it is taken regularly for 2-3 days. This drug is generally safe but may cause gastric irritation and can make asthmatics worse.This type of drug can also be used as a gel and can be applied topically over the painful area. Ibulieve and Voltarol gel are two examples and can be very effective, particularly where the inflamed joint is close to the surface (eg elbow). The gels can be used in addition to the tablet form of the drug.
Preparations such as Glucosamine may have some use in the treatment of early arthritis. These donot work in the short term and are not recommended for the treatment of symptoms brought on during Bisley week!
Other sources of professional help
Pharmacist:
All pharmacists can offer advice for simple medication treatment of orthopaedic problems; often a very useful source of assistance.
Physiotherapist:
There are many very good independent state registered physiotherapists, excellent professional practitioners who can advise and undertake treatment for a wide range of conditions.
Chiropractic:
Similar to physiotherapists, these practitioners are trained predominantly to deal with trunk conditions, and will emphasise the importance of spinal alignment.
Osteopath:
For any musculoskeletal problems, concentrating on manipulation and massage techniques.
Sports therapist:
Not as strictly regulated as the above, but can be very effective. Do ensure any therapist you consult for treatment is registered with their professional body and if possible always try and obtain a personal recommendation (just as you would, of course, before consulting an orthopaedic surgeon!)
